The number of young people changing gender has risen fast in the past decade. What’s going on – and should we be celebrating or concerned?

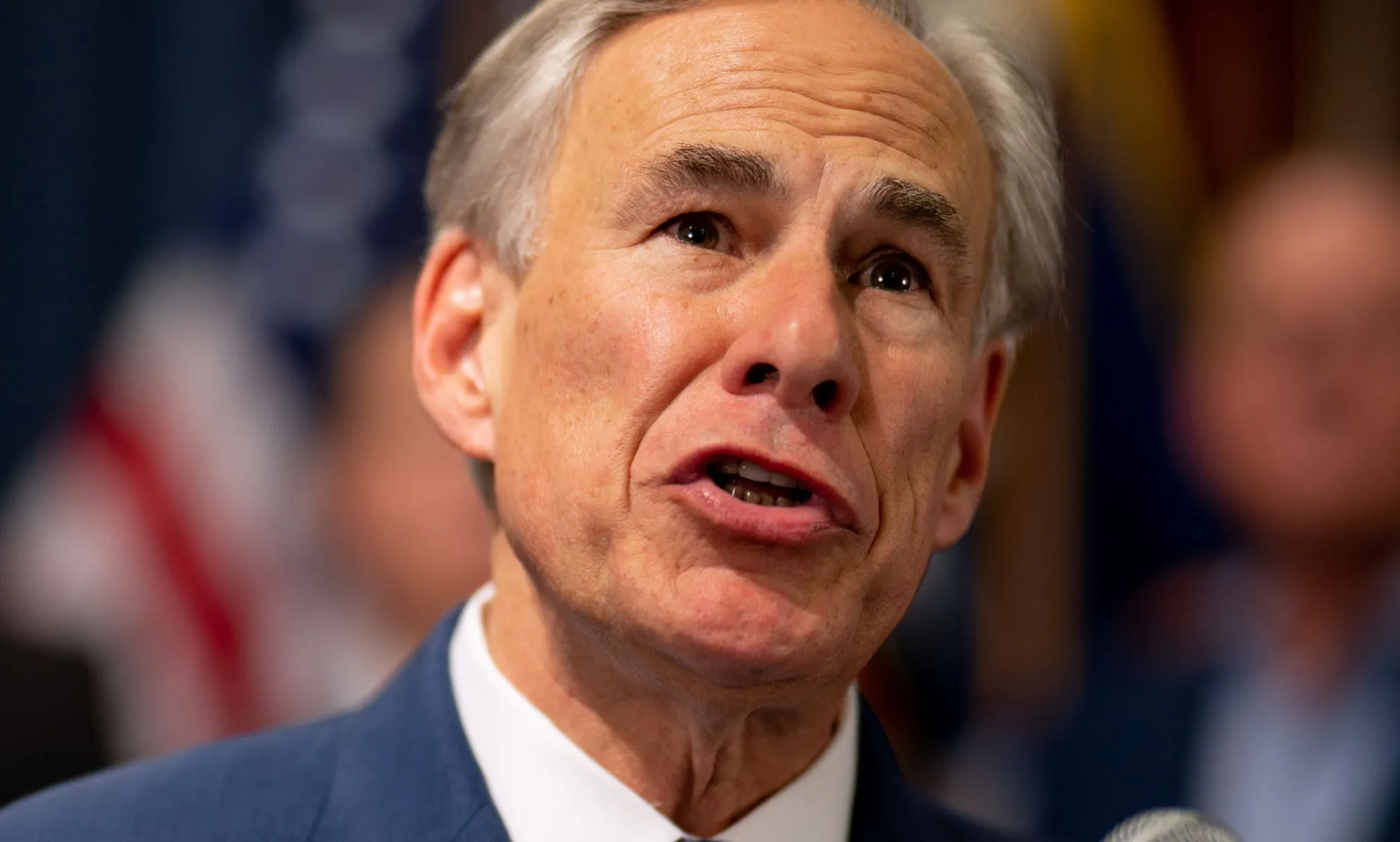
In 2011, eight young people sought medical care at the gender clinic at the Royal Children’s Hospital in Melbourne, that treats eight- to 16-year-olds. By 2021, that number was 100 times higher at 820. The fastest growth has been among adolescent girls. Credit: Stocksy
Misha* slouches in a computer chair and looks at me wearily, struggling to find an answer to my question.
“It brings up deeply rooted …”
The words trail off, then begin again, “… disgust, fear.”
Misha hunts for the words.
“It brings up pain – unbelievable amounts of pain.”
We’re in the dining room of an ordinary weatherboard house in an inner Melbourne suburb, and early spring air is seeping inside. Misha, mousy hair parted in the middle, wearing a lumpy lumberjack coat and baggy T-shirt, shifts uncomfortably. Dinner is growing cold on the table. Misha’s mother, Steph*, watches the struggling teenager intently.
We’re talking about gender. Misha, born, named and raised a girl, has since early high school had a powerful desire to be a man. About an hour into our interview, I’ve asked what, specifically, is causing such intense self-hatred. Misha cannot answer. Just that it hurts.
Misha and Steph, a single mother, are both exhausted. Steph works casual jobs and as a freelance designer to keep her little family together after her marriage broke down 12 years ago, and for five of those years gender has been the dominant, angst-ridden conversation. In Steph’s telling, before it all went wrong, Misha had been a “happy, happy, shiny kid, confident and chatty”.
“I was pretty happy as a primary-schooler,” Misha concedes. “It wouldn’t have lasted. If my childhood was a bit more difficult I might have been more prepared.”
When Misha was 12, Steph contracted a life-threatening illness, which deeply affected Misha, who was also dealing with as-yet-undiagnosed autism and trying to negotiate the tricky first few months at an inner suburban high school. Misha made a deep but troubled friendship with a quirky, charismatic girl, who announced she was bisexual, then non-binary. Their only subject of conversation was gender: “All of my knowledge about it came from her.”
“My body was getting worse. It felt like it was poisoning itself.”
Misha*
There was also “a lot of propaganda around” at school, Misha says, from “my peers, posters, school counsellors” and a “queer” space to gather in. Then puberty hit.
“We started talking about trans identities and I thought, ‘This could be me.’ My body was getting worse. It felt like it was poisoning itself.”
Misha’s friend soon moved on and now identifies as a girl again, but Misha could not. By the senior years of the “arts, social justice” stream of Misha’s public school, only a small handful of students in Misha’s class of about 20 said they were “cis-het” – heterosexual and identifying as the gender that corresponded with their birth sex. Everyone else adopted one of multiple labels. “Being cis-het was very uncool because it’s boring,” Misha says. “Also, they want to feel oppressed and special … The last thing you want to be is ‘privileged’.”
Misha is sceptical about many of their gender claims and finds it “cringey” when pronoun use comes up. “Having to call people by pronouns that are just not the same as what you see in front of you is like being in someone else’s idea of reality.” (So awkward is it that I’ve avoided using any pronoun for Misha, a line Steph treads every day.) Despite this scepticism, Misha remains plagued by gender distress, known as gender dysphoria.
“I don’t want to be in this position. I don’t believe in the ideology,” Misha tells me, “but I have very serious dysphoria now and can’t make it go away. If I did believe it all, I’d say I identify as a male: I hate talking because I don’t like hearing my voice; I don’t want people to hear it because it sounds feminine. I hate that I’m small.“
When Misha tried to share this internal conflict with friends on a social media chat, they shut the conversation down, saying Misha was a conspiracy theorist, “transphobic” and that Steph was a toxic influence who should be rejected.
The whole subject blindsided Steph, who’s having to make it up as she goes along. She helped Misha at about 14 to socially transition – to present to the world as a boy. She bought chest-binders after she realised Misha was using packing tape. Steph also facilitated Misha adopting a non-gender-specific name. Steph still struggles to say it.
But from Steph’s point of view, each time she accommodated the dysphoria, Misha’s mental health notched down. Misha was self-harming, depressed, had anorexia and a profound disinterest in school. Even so, a succession of psychologists and doctors wanted to focus only on gender affirmation and medical treatment: “Trauma and autism never got a look-in.”
“I feel like I’m in a horrible bind where I’m torturing my kid.”
Steph*, Misha’s mum
Steph drew the line at helping Misha access cross-sex hormones. These medications – oestrogen and anti-androgens for children born as boys, testosterone for those born as girls – make young people’s physical form more closely resemble their gender identity. Some changes are irreversible: with testosterone come a deeper voice, more facial and body hair, the possibility of male pattern baldness, and with oestrogen comes breast growth.
“I feel like I’m in a horrible bind where I’m torturing my kid,” Steph says. But overriding that is a greater fear: that Misha would regret decisions made now. Misha, too, fears the physical and health consequences of taking hormones.
Now 18, Misha is eligible as an adult to seek private hormone therapy without Steph’s consent. Having seen friends turn 18 and start hormones, Misha is appalled at the idea of being a woman but wavers – daily, sometimes – on the next step. “All the people I idolised in the media were men – why can’t I be like them? It was a 50/50 chance. Why did I have to end up like this?”
If hormones are on Misha’s horizon, Steph will not stand in the way. And she will be there on the other side. While Misha’s dad is regularly in contact, Misha chooses to live with Steph. As troubled as it is, their relationship is warm, full of affection and care, along with frequent bursts of laughter. “The only thing keeping me alive is the love of my family,” Misha says. “Mum and Dad.”
In suburbs and towns across Australia, and throughout the Western world, households are talking intensely about gender as families grapple with something that feels entirely new, and big. Starting in about 2012, a surge of people – many of them children and adolescents – began coming forward to say their gender was incongruent with their birth sex.
Some of these young people are content to dress ambiguously and perhaps change their name, to identify as non-binary or by one of a panoply of different genders, and ask for different pronouns. Some live like this for a time, then revert to their birth gender. A proportion, though, seek medical treatment.
The numbers tell the story. In 2011, eight young people sought medical care at the gender clinic, at the Royal Children’s Hospital (RCH) in Melbourne, that treats eight- to 16-year-olds. By 2021, that number was 100 times higher at 820. The fastest growth has been among adolescent girls. A publicly funded clinic for over-16s at Monash Health also saw a steep rise – a phenomenon also reflected overseas. But Victorian government figures show numbers at both the Royal Children’s and Monash have fallen markedly in the past two years, to 634 at the children’s hospital last year and just 327 to the end of October.

Credit: Royal Children’s Hospital, Victorian government.
The state health department did not offer an explanation for the recent decrease, just as nobody can explain with confidence what caused the increases. Some research postulates that the huge rise might be partly due to an increase in trans visibility in the media and a reduction in the stigma involved in being transgender. Sceptics argue there might be an element of “social contagion”, particularly among teenage girls, an argument the trans community vehemently rejects.
There are publicly funded gender clinics in all of Australia’s mainland capital cities, but the clinic at Melbourne’s RCH is the biggest and, under its former long-time head, former Olympic gymnast Dr Michelle Telfer, led the national response. In 2018, a team led by Telfer published standards for the treatment of gender incongruence and dysphoria in children and adolescents which guide clinics around Australia. Recognised globally, they’re based in large part on material including influential reports emerging from pioneering Dutch gender clinics in the 2000s, as well as on guidelines from the World Professional Association for Transgender Health. The model is known as gender-affirming care.
Affirming care starts from the premise that a child’s statements about their gender identity should be taken seriously and acted upon. In the words of the Australian Professional Association for Trans Health (AusPATH), “trans patients are the experts of their own lives and the final authority on their own gender”.

Dr Michelle Telfer the former head of Melbourne’s Royal Children’s Hospital’s gender clinic.Credit: Simon Schluter
At the adolescent clinics, treatment is slow, careful and multidisciplinary. Many drop out when they confront the waiting list and the reality of treatment, but if they persist, the first stage of treatment is to prescribe drugs known as puberty blockers, which can be given to children at the early stages of adolescence – when breasts are budding on girls and testes starting to grow in boys – to suppress further physical development. The rationale is to give a child and their family time to think. The child might stay on puberty blockers for several years and the effects, the hospitals say, are entirely reversible, though this is disputed.
The next step is cross-sex hormones – oestrogen and testosterone. At each stage, according to Family Court of Australia rulings, the clinic must obtain the consent of both the child’s parents as well as clinicians. The third stage, “top surgery” to remove breasts, is very rare for adolescents in Australia; “bottom surgery” to change genitals is only available to adults and only if they can afford private treatment. Advocates of these treatments say the science is settled: they prevent suicides and self-harm, and to delay or withhold them is unethical.
Many families agree and happily support their child’s transition, and affirming care has the support of most doctors, psychologists and psychiatrists. Increasingly, though, some are speaking up against it.
In the United Kingdom, London’s Tavistock children’s gender identity clinic will close down next year after an official review questioned its methods. Britain’s National Health Service responded by saying its gender services would only prescribe puberty blockers as part of formal research studies. Public clinics in parts of Europe are becoming manifestly more conservative too, and the clinic at Sydney’s Westmead hospital in 2021 produced a controversial study of 79 patients that declared many of the young people it was treating “did not have the cognitive, psychological, or emotional capacity to understand the decisions they were making” in the context of the potential impact on their fertility, sexual function and brain development.
Internal divisions at Westmead subsequently slowed the clinic’s work to a crawl, and the report and its authors came under significant public pressure. Professor Ashleigh Lin, the president of AusPATH, said it was now under new leadership and back on an affirming-care track. As for the more cautious approach being taken by UK and some European clinics, Lin, a youth mental health researcher, insists they came under the sway of an “anti-child and -adolescent-affirming lobby”.
The Victorian clinics at RCH and Monash rarely give interviews about their work and were not available to address these questions. The Victorian government also refused to answer questions from Good Weekend about details of the clinic’s work, citing privacy concerns.
But internationally, and among some doctors and scientists in Australia, the reassurances that affirming care is the best possible treatment are not being taken at face value. The Royal Australian and New Zealand College of Psychiatrists is revising its position statement after disquiet from some professionals, and one medical insurer has withdrawn GP cover for some treatments. A small number of legal challenges is finding its way into the courts, and groups, led by politicians and a number of vocal doctors and lawyers, are agitating publicly for a rethink.
The struggles of people like Steph and Misha are real, but they are not the only story. In another weatherboard home in Melbourne’s middle-ring mortgage belt, Sage Moorhen is happy, balanced and in love.

Sage Moorhen (front right) with partner Priya, and his parents Sue and Scott (at back). Sage told his parents he was transgender at 17 and asked for their support.Credit: Chris Hopkins
Sage is typical of the new transitioners. He was, in the parlance, assigned (or presumed) female at birth but decided, or realised, during adolescence that he wanted to be a man. At 22, he has been taking testosterone – known colloquially as “T” – for three years and has recently had “top surgery” (breast removal). He is not, at this stage, seeking any further surgery.
I’ve known his family for years. They are good friends. I knew Sage when he was a sweet, quiet girl who wore overalls most days. I had not seen him for a few years, so when I walked into a cafe for our first interview, his transformation was so profound I did not initially recognise the sweet, quiet man sitting in the corner.
He “passes”. Looking masculine has made him feel more secure walking the city streets at night – something he feels guilty about. It’s also made him comfortable dressing flamboyantly. At our meeting he’s wearing a green paisley shirt, sparkly gold Doc Martens and multi-coloured glasses. His voice is a light tenor and he sports stubble and longish hair in a man-bun.
Later, over family dinner, I join him at a crowded table with his parents, Sue and Scott, his sister and brother, and his partner, Priya. Priya identifies as non-binary and gender fluid – they shift between male and female, and neither – describing their gender as “floating through space and drifting towards planets”. The couple are planning their wedding.
Looking back, Sage dates his feelings of gender incongruence to primary school, where he had no friends and “a distinct feeling of otherness”. Much later he was diagnosed with autism, but at the time he just thought the “girls were catty and the boys were dickheads”.
Sage is five years older than Misha, and at his private secondary school, the gender-affirming posters had not yet hit the noticeboards. When the subject of sex and relationships came up in year 8 and 9, it felt like a foreign country. “I did a lot of Googling and started stumbling on the queer community … it was the first time I’d come across an alternative to being heterosexual.” In year 10, in 2017, Sage came out as lesbian. Later he was non-binary – “a safe, experimental space” for him.
“As a parent, you have the responsibility to look out for your kids.”
Scott, Sage Moorhen’s dad
Finally, at 17, Sage told his parents he was transgender and asked for their support. Sue, a practising (though not doctrinaire) Catholic, who works in a finance company, wanted six months to think about it. She was worried about the irreversible physical changes of gender affirmation.
The turning point came a year after Sage’s declaration, when Sue and Scott sat down with him at an appointment with his psychologist, gender specialist Ben Callegari. “As a parent,” says Scott, “you have the responsibility to look out for your kids.” He went into the meeting thinking they all needed more time to think.
Callegari convinced them otherwise. “Transition,” he tells me, “is to do with autonomy and identity development. Our job is not to tell someone who they are, what they are, what to do. Our job is to help them make decisions for themselves.”
Walking out of the meeting, Scott says, “I thought, ‘I’ve just been hit by a velvet brick.’ It was a pretty big moment for all of us, but after that meeting I was comfortable.” Says Sue: “We used to have two daughters and a son. Now we have two sons and a daughter,” and adds, joking, “I’m just jealous that Sage beat me through menopause.”
“It was a relief I didn’t have to try so hard anymore.”
Sage Moorhen
Sage says the potential side- effects were laid out carefully, including that a deeper voice and extra body hair were likely irreversible. Fertility was talked about a lot and he was told that, given the uncertainty of some outcomes, he could have eggs harvested or, if he wanted to have children, it was likely still possible while he was young. He also looked at adoption as a back-up. But, without transition, he believes he would have been at greater risk of suicide: “It’s my wellbeing right now that I’m thinking about, rather than the wellbeing of the kids I might have some day.”

Sage Moorhen: “It’s my wellbeing right now that I’m thinking about, rather than the wellbeing of the kids I might have some day.”Credit: Chris Hopkins
Sage says he feels good on testosterone, relaxed. “I realised I’d been putting so much effort into looking this way, holding myself this way, and it was a relief that I didn’t have to try so hard any more. I nearly cried but then I realised my tear ducts had stopped functioning.” Some trans men say testosterone makes it harder to cry.
Sage did have some self-doubts and sleepless nights, but having both medical and family support reassured him. “The job of the medical professionals was to make me safe; my parents and friends were just there to make me happy.”
In another lounge room, in a cosy apartment in the heart of progressive, metropolitan Melbourne, I meet a group of parents who are desperate to have a more open discussion about what they see as the tragedies happening in their lives. There are about 15 people here – representative of a wider support group of 30 – and all their children are expressing gender incongruence.
These are middle-class, middle-aged professionals. They have grey hair and serve nice cheese and go to jobs in law firms and universities and schools. This apartment is in the electorate of Greens leader Adam Bandt and they would fit right in, except they say the left has abandoned them on this issue. Their gender-questioning children are mostly born female and are neurodiverse, and live with mental health issues. In this group, they insist on referring to their children by their birth sex – what the trans community calls misgendering them. To these parents, the real threat to their children’s physical and mental health is affirming care itself. They say they oppose it out of love.
They ask to remain anonymous because they fear being publicly labelled anti-trans, or transphobic, their jobs even threatened. “My own child thinks we are the Antichrist here,” says one father, Tony*. These parents believe their children have arrived at their new gender identities with no forewarning and based on a trend. They see most of the media as complicit and the law in Victoria as threatening. Under Victoria’s 2021 Change or Suppression (Conversion) Practices Prohibition Act, taking active steps to stand in the way of any person’s desire – even a child’s – to affirm their new gender is an illegal conversion practice (subject to up to 10 years in jail for cases of serious injury). By contrast, facilitating their transition is, according to the Victorian Human Rights and Equal Opportunity Commission, “completely legal – and encouraged”. The ACT has a broadly similar law and NSW is contemplating one. Queensland only holds medical professionals liable for prosecution in gender-suppression cases.
Tony and Jane* were asked if they would prefer a live son or a dead daughter. They did not return for the second appointment.
These parents call the legislation the “anti-therapy law” – they say it’s spooked mental health professionals into believing that when a child mentions gender, they must affirm it or risk prosecution. Finding a “neutral” therapist for their troubled, anxious, loner children to deliver “exploratory” or “watchful waiting” therapy is now a minefield.
They see what they call “gender ideology” wherever they look. In their eyes, the posters and flyers at schools designed to promote acceptance act instead as propaganda. Six children of parents here transitioned socially to another gender at school – changing dress, pronouns, even names – without their parents’ knowledge. It happened under a policy called “mature minors” where, if school authorities deem a young person intelligent and mature enough, they can make some decisions for themselves.
Andrea* says three of her daughter’s four schoolfriends “turned into boys” in year 8. In year 9, their daughter followed suit. Andrea’s husband, Michael*, describes their child’s 18th birthday party as “five penis-less boys dancing and singing and baking each other cakes”.
Tony says his daughter, who is autistic, was suffering anxiety, obsessive compulsive disorder, vomiting and bullying at school, but when he and his wife, Jane*, took her to a psychiatrist and “the gender issue came up”, they were referred to the Royal Children’s Hospital gender clinic. There, Jane says, a clinician said they could help their 14-year-old daughter find her “real” gender, and raised the prospect of suicide if they did not: Tony and Jane were asked if they would prefer a live son or a dead daughter. They did not return for the second appointment. Their child started testosterone at age 18 and, Jane says, is now “performing a boy stereotype” without really knowing what a boy is.
Tony says these issues are hard enough to deal with but, “it’s making it worse that we can’t talk about it … we have to embrace gender ideology. And if you don’t you are a right-wing nutjob.”
Les* agrees that, for them, autism, trauma from sexual abuse and gender are tangled together, which they are dealing with in therapy.
Another parent, Monica*, tells me that, at 17, during a COVID-19 lockdown, her child gave her a speech out of the blue: “I’m a boy. I want a mastectomy and testosterone.” The child, Les*, is autistic and suffers trauma from sexual abuse as a child. Les tells me they’d always felt uncomfortable with aspects of being female – particularly their voice, their breasts and menstruation – and had latched onto the idea of becoming a transgender man at school, along with five or six others in their year level. Their art shows the pain of feeling caught in a confusing gender binary.
Now, at 20, after a great deal of “neutral, exploratory” therapy that Monica curated to avoid gender-affirming therapists, Les says they no longer want to take testosterone. Removing their breasts is still “on my plate” but not a high priority. They agree that, for them, autism, trauma from sexual abuse and gender are tangled together, which they are dealing with in therapy.

Artworks by Les*, 20, depicting their dissociation.
Resisting the gender-affirming approach cost one parent their job after, traumatised by what was happening at home, they had a tearful outburst in the face of material being displayed at work. Others have lost their relationships with their children and their extended families. I ask, wouldn’t it be better, healthier, if they agreed with the doctors and psychologists, the trans community, the family support groups and clinics, the Victorian law and the zeitgeist, and simply affirmed their children’s chosen gender?
Tony cannot contain his grief and sadness. “I call my kid the new name and I pretend that she’s a boy and I guess that’s probably what you mean by ‘affirming’, but no one ever talks about what that means, because affirming really means telling her to hate any female characteristics,” he says. “It’s so negative. It’s about hating their body. Hating their past. Hating their childhood. Hating how people see you … and loving a gender stereotype … it doesn’t create anything. It destroys this curious, lovely, beautiful little creature that we had. It’s terrible to watch … We do all that stuff and we have lost this beautiful child to this terrible, terrible ideology.”
The course of Mel Jefferies’ life is precisely what frightens these parents. Born female, and living with a number of mental health issues, from age 16, she was affirmed as a trans man by doctors, the trans community and mental health professionals. For years, on and off, she took testosterone, she’s had a double mastectomy and now at 32, she bears the physical scars of regret.
Mel says she’s been questioning her gender and sexuality for half her life but now describes herself as a “detransitioner”. When she looks in the mirror, for the first time she sees herself as a cis-het woman. And she’s angry. “I thought transitioning was a panacea for all my problems, but it’s compounded them.”
The worldwide literature on trans “regret”, or detransition, suggests people like Mel are a small minority – perhaps one per cent of those who transition.

Mel Jefferies believed that transitioning would be a panacea
for various mental health issues. “It’s compounded them,” she says. Credit: Chris Hopkins
I speak to a handful of detransitioners for this story – two of whom are either suing or considering suing their medical practitioners – but it’s true that few have come forward publicly in Australia. Sceptics of affirming care say it might take 10 years for people to admit to regrets but that we will see more – and more lawsuits. One large medical insurer is already taking precautions. In July, MDA National, one of the biggest providers of medical indemnity insurance in the country, stopped covering practitioners who assess or treat people under 18 for gender reassignment. Its president, Dr Michael Gannon, said, “We don’t think we can accurately and fairly price the risk of regret.”
In the US and the UK, detransitioners have become influential voices in a growing debate and have swayed public and official opinion. Mel is becoming an advocate in Australia for more caution. She has appeared on TV and recently addressed a forum in Victorian parliament with a number of doctors and lawyers as they lobbied for an upper house inquiry into affirming care for adolescents. That bid failed when the government and crossbenchers voted against it. The last time this was considered officially was in 2019, when then-health minister Greg Hunt asked the Royal Australian College of Physicians to conduct a review. One of its conclusions was: “Withholding or limiting access to care and treatment would be unethical and would have serious impacts on the health and wellbeing of young people.”
Mel tells her story in bursts of words punctuated by a twitch of her head and the occasional self-conscious laugh. She’s only working it out herself after seeking her medical files, which run to almost 20 folders, spanning multiple organisations and experts and mental health diagnoses. She has eating disorders and body issues, anxiety and depression and has self-harmed. Her most recent diagnosis, provisionally, is autism.
The short version is that a number of sexual assaults – her first as a teenager by a female schoolfriend – gave her a hatred of her body and a desire not to be female. At 16, she was introduced to the notion of a transgender identity by an online community and at 18, after a one-hour consultation, a psychiatrist in Sydney concluded there was no psychiatric reason not to proceed with hormones. Her relationship with her family was already strained and the trans identity drove a further wedge between them. Mel moved to Melbourne where she believed she could begin her transition faster and, for the next two years, took testosterone.
Mel was a young adult when she embarked on this path. She did not go through the public gender clinics and made her own decisions. But she says she was vulnerable and under the sway of a medical diagnosis that convinced her that hormones could fix her. “It was such a toxic idea for me,” she says.

Credit: Adapted from Australian Standards of Care and Treatment Guidelines for Trans and Gender Diverse Children and Adolescents, the Royal Children’s Hospital, Melbourne.
In 2013, she publicly described herself for the first time (on SBS’s Insight program) as a detransitioner. Later, though, reassured by friends in the trans and gender-diverse community that feeling unsure was normal, she started testosterone again. She said it was hard to speak up about doubts within the community because of the danger of being labelled transphobic.
“It’s like chasing the dragon. You get a real high from it and then you start to feel bad and you need to have more.”
Detransitioner Mel Jefferies on a onetime desire for more surgery
At 26, still struggling with body image issues and rage at her female form, Mel had her breasts removed. Immediately, her focus turned to her thighs and stomach, and to the desire for more surgery, including a full hysterectomy. “It’s like chasing the dragon. You get a real high from it and then you start to feel bad and you need to have more.” She did not go through with that procedure but the mental health problems persisted, compounded now by phantom pain from the double mastectomy, scars, and what she describes as “zipper tits” and a “pepperoni nipple”. She is on a disability support pension and struggling to afford the electrolysis to remove the hair that grew on her “face, back and chest, my stomach and butt” as a result of testosterone.
I ask Mel how her life feels. The question catches her at a vulnerable moment. “It feels like I’m dunked into the ocean and can’t figure out which way is up. I can’t get air. And people are laughing at me because I don’t know how to swim.” The community she was once part of has been no help: it “love-bombed” her when she wanted to transition but she says has dismissed her since she detransitioned.
Professor Ashleigh Lin, the president of AusPATH, acknowledges there is “some stigma” against detransitioners and her organisation is working hard to change it. She insists, though, that a small number of their voices are being overblown in the media and by some politicians to damage trans people.
Retired clinical psychologist and sex therapist Sandra Pertot, who has almost 50 years’ experience, argues that minimising the experience of detransitioners is precisely the wrong approach: “These people should help us develop a safer diagnostic process … I don’t care how small a percentage they are … it’s straight science.”
As the number of people presenting as trans has jumped, so have the political concerns. The scientific evidence either way is limited and each side questions the other’s methodology and conclusions. Even the language is contested: are you a man or woman, or were you assigned – or more recently “presumed” – female or male at birth? Politicians are sometimes asked, as a trick question, “What is a woman?”
Elite sporting competitions globally have grappled with the issue, particularly of transgender women competing – an issue Senator Jacinta Nampijinpa Price says will be her next project. All-gender toilets are (controversially) being opened at some schools. It’s been destructive in parts of the left, which is torn between feminism’s insistence on unique and safe spaces for females – domestic violence refuges, toilets, even prisons – and the newly asserted right of transgender women to use them.
Members of the Greens have been ejected from the party over these questions. Labor has adopted affirming care as a policy but the Liberal Party is struggling as controversial candidates such as NSW’s Katherine Deves and Victorian upper house MP Moira Deeming attract support within the party but controversy outside it. Deeming’s presence at a March rally gatecrashed by neo-Nazis created a nightmare for her leader, John Pesutto, that he cannot wake up from.
Much is contested, but what’s not is that young people with gender incongruence and dysphoria are multiple times more likely to be autistic than the general population. They also have mental health issues on a broader scale. An 859-respondent online survey of the Australian trans and gender-diverse community, Trans Pathways, published in 2017 and cited in the Royal Children’s Hospital treatment guidelines, found three-quarters of trans and gender-diverse people say they’ve been diagnosed with depression and anxiety, one-fifth with a personality disorder and almost a quarter with an eating disorder. Four in five self-harmed.
Advocates of affirming care insist that mental health distress is driven by barriers to accessing healthcare and by discrimination, and that treatment relieves that. Studies now coming out of gender clinics “show the benefits of gender-affirming care, including hormones”, says AusPATH CEO Lin. Detractors say the evidence of that is thin and that addressing gender dysphoria can come at the expense of treating other conditions such as depression, anxiety and autism.
Then there is the most sensitive subject of all: suicide. Four in five respondents to Trans Pathways said they’d had suicidal thoughts and almost half had tried to kill themselves. It’s impossible to know how many die by suicide. A Victorian coroner’s report last year noted police do not routinely collect gender identity details at scenes of suicides, and some who take their own lives might not have declared their trans identity. Sceptics of affirming care say the risk is overstated and used by some to stifle legitimate questions. A study published in 2020 surveyed 40 years of information about gender-dysphoric adults and children at an Amsterdam clinic and found deaths by suicide were rare, but still three to four times higher than those in the broader Dutch population.
Within this most sensitive area, Victorian coroner Ingrid Giles will hold an inquest starting on Monday into an all-too-real cluster of five young transgender or gender-diverse people who took their own lives during Victoria’s long season of lockdowns. Their stories are complex: opening statements in October noted all five had serious mental health issues, including feelings of social isolation, and all “had been commenced on gender-affirming hormone therapy”.
Sensitivities in the trans community about increasing the risk of suicide have led to a reluctance to engage in any public discussion that they believe disputes their right to exist – preferring to advocate for improved treatment options behind the scenes. In a recent National Press Club speech, trans pioneer and former Neighbours actor Georgie Stone criticised journalists for using “dehumanising, clickbait catchphrases like ‘the trans debate’ “. Asked what she’d say to those seeking to ignite a culture war on the issue, Stone replied: “Stop trying to kill us.”
“I wish I’d been able to transition when I was, you know, 10 or 11 or 12.”
Michelle McNamara, volunteer chair of Transgender Victoria’s advocacy committee
It’s taken some convincing to get Michelle McNamara, the volunteer chair of the advocacy committee at Transgender Victoria, to agree to an interview for this story. Like many in the trans community, she is wary of the media and anything that’s likely to deter or mislead “any [child, parent or adolescent] … from seeking professional advice and healthcare”.

Michelle McNamara and Son
Vivienne from Transgender Victoria.
Michelle lived for decades with gender suppression and suicidal thoughts.Credit: Chris Hopkins
Michelle and Transgender Victoria’s chief executive, Son Vivienne, speak for the longer view. Both trans themselves, they say gender diversity has always been among us but suppressed by prejudice, and the affirming-care model supports them in the face of that. These gains are now under challenge from an “avalanche of disinformation”, Michelle says.
Asked about parents confronting the issues raised in this story, she says: “If those parents really loved their children, they would be going hell for leather to help them affirm their bloody gender.”
Michelle has been trans her whole life but says she was forced by stigma and ignorance to live six decades as the wrong gender. This year she celebrates a triple anniversary: her 70th birthday, 40 years of marriage (to Barb) and 10 years as a transgender woman. One of her earliest memories, she tells me over lunch in their sun-drenched lounge room in Melbourne’s north-east, was, at the age of about seven, dressing up in women’s clothes, shoes and make-up, and “thinking I was terrific”. Immediately following were feelings of guilt. “I knew somehow at that stage that it was wrong … I knew I had to keep it secret.”
Puberty, and a growth spurt that made her 182 centimetres at the age of 11, stopped any fantasies she had of living life as a woman. And anyway, until she saw an Australasian Post magazine in the barber’s shop in 1966 – featuring legendary Sydney transgender performer Carlotta – she believed she was the only person like her in the world. But the Kings Cross club scene was a million miles from suburban Melbourne, “and I sort of said, ‘That’s not a world that I can aspire to.’ ” So Michelle “packed it all away”.
As she lived life and built a career in science as a man, suicidal thoughts were her companion, a result of the “deep scarring from seeing the abuse, the ridicule, and the psychological and physical violence that they heaped on transgender people all my life”. The long gender suppression damaged her, too: “I think it closed me … made me emotionally distant and quite angry as well.”
Finally, at 60, she decided to transition when, studying Buddhism, she began letting go of the male parts of her gender identity and embracing the female. “I wish I’d been able to transition when I was, you know, 10 or 11 or 12, when I was having those feelings.”
“Our lives,” says Transgender Victoria’s CEO Son Vivienne, “are an invitation to see beyond the binaries.” Vivienne grew their first beard this year and has been in both straight and lesbian relationships. They now identify as non-binary and queer. They have raised two (now teenage) children, mostly as a single parent, and describe it all as “perfectly unregrettable parts of myself that helped me grow into who I am now”.
That said, there is “no trans person in the world who will tell you that gender affirmation is a magic wand or fix for all discontent”, and while stigma persists and “our wellbeing remains a subject of ‘debate’ ” it will remain complex and difficult, Vivienne says. Transgender Victoria tries to address this by providing social and community connection and support.
Vivienne urges parents opposing the gender transition of their teenagers to “encourage the young person’s courage and curiosity … let them know that they are loved regardless of what pathway they take, and leave space for them to grow and change”, adding that plenty of trans people “come on and off hormones through their lives”, that breasts can be reconstructed and body hair removed or lived with.
I have spoken to more than two dozen people for this story – trans people and people who’ve regretted their transitions, anxious families, doctors, lawyers, researchers and advocates. One view holds that affirming care is working well and the most important problem is discrimination against trans people; critical questioning of these things can lead to mental health harm and suicides. The other argues that society must ask more serious questions about who we are treating and how – that despite the safeguards built into the public clinics, we are choosing a cohort of young people for treatment too indiscriminately and doing “iatrogenic” harm – damage caused by medical procedures.
At times during my research, representatives of both views approached me to ask what I thought could possibly motivate the other side. Neo-Nazis and the hard-core culture warriors aside, my observation is that both want the best for children and young people, but they genuinely disagree on what that is and how to achieve it. Some think the current medical model is harmful, while others fear that retreating from it will take us back to the bad old days.
Gender fluidity is here to stay. That genie is not going back in the bottle. But we need to be able to talk more openly and with more nuance about these questions, with the human beings involved at the centre.
Vivienne does not retreat for a moment from affirming care, and will not engage in a discussion where “our right to exist is disputed”. They do agree with one thing, though: “We need to listen better to young people and older people and ‘confused’ people and ‘people who change their minds’ so that we can understand the complexities and care better for everyone’s needs as they unfold throughout their lifetimes.”
* Names have been changed.
Lifeline 13 11 14; Kids helpline 1800 55 1800
To read more from Good Weekend magazine, visit our page at The Sydney Morning Herald, The Age and Brisbane Times.